以下文章轉(zhuǎn)載自:
American Journal of Neuroradiology
Presurgical Mapping with fMRI and DTI: Soon the Standard of Care?
The technique of fMRI has been around for over 30 years, and DTI for about 15 years. The first application of fMRI was by Ogawa et al, in 1990. In a rat model, this team was able to manipulate the blood oxygen level–dependent (BOLD) signal by inducing changes in deoxyhemoglobin concentrations with insulin-induced hypoglycemia and anesthetic gases. About a year later, Kwong and Belliveau published the first images of cerebral areas that responded to visual stimulation and vision-related tasks.
DTI was first described by Basser et al, who were experimenting on a voxel-by-voxel characterization of 3D diffusion profiles, which took into account anisotropic effects (instead of eliminating them, as in standard DWI). Tractography (or fiber tracking) was developed by applying statistical models to DTI data to obtain anatomic fiber bundle information.
Although both fMRI and DTI are now currently available in most scanners, well beyond the framework of academic institutions and research protocols, these techniques are not quite considered “standard of care.” Indeed, the processes that govern the translation of new technology into clinical practice are complex. Even more complex are the processes that lead to establishing clinical practice as standard of care, particularly at a time when established patterns of care delivery are being increasingly challenged and economic difficulties affect all aspects of society, certainly including health care.
However, some challenges, especially with fMRI, go back to basic cerebrovascular physiology. The cerebrovascular response to neuronal activation, also referred to as “functional hyperemia,” was first recognized in 1890 by Roy and Sherrington, who initially proposed a metabolic hypothesis to the phenomenon, ie, mediation via release from neurons of vasoactive agents in the extracellular space. The major role of astrocytes as key intermediaries in the neurovascular response — being interposed between blood vessels and neuronal synapses via their foot processes as modeled in the “tripartite synapse model” of the neurovascular unit — has since been recognized. Although complex, astrocyte response to changes in synaptic activity is primarily mediated by glutamate receptors through changes in intracellular Ca2+ concentration.
In fMRI, contrast is based on the BOLD effect, which reflects local shifts of deoxygenated-to-oxygenated hemoglobin ratios due to local increases in blood flow in excess of oxygen utilization following brain activity. As a result, the foundation of the fMRI BOLD signal is based on local changes in cerebral blood flow that are not linearly related to the metabolic changes inducing the flow change.
Therefore, BOLD fMRI rests on 3 major approximations: 1) the technique does not directly reflect neural activity, ie, generation and propagation of action potentials, synaptic transmission, or neurotransmitter release/uptake; 2) the changes in BOLD signal originate from that portion of the vasculature experiencing the greatest change in oxygen concentration, which occurs in the venules in the immediate vicinity of the active neurons; and 3) more importantly, fMRI signal relies on intact “neurovascular coupling,” the phenomenon that links neural activity to metabolic demand and blood flow changes.
The main reason fMRI is clinically useful most of the time is that under most circumstances neurovascular coupling remains fully intact, unaltered by confounding disorders that can interfere with this relationship. However, it has long been known that neuronal activation results in local blood flow increases that exceed local oxygen consumption, so that the oxygen utilized may constitute a small fraction of the amount delivered. Under normal conditions, the oxygen concentration in draining venules increases during neuronal activation. The original researchers who discovered this phenomenon named it “neurovascular uncoupling” or “neurovascular decoupling.” From a medical perspective, “uncoupling” or “decoupling” implies a pathologic condition, suggesting something abnormal about tissue that demonstrates this phenomenon. More recently, researchers have preferred the term “functional hyperemia” to describe the phenomenon. In fact, when there is interference with the mechanism producing functional hyperemia, the term "neurovascular uncoupling" has been re-applied, albeit with a completely opposite meaning from that originally used. Impairment in the flow response leads to neurovascular uncoupling and a reduced BOLD signal in response to neural activity, which can lead to false-negative errors in fMRI maps.
John Ulmer, reporting on a series of 50 patients, found that although accurate cortical activation could be demonstrated most of the time, various cerebral lesions could cause false negatives in fMRI results when compared with other methods of functional localization, suggesting contralateral or homotopic reorganization of function. He further suggested that pathologic mechanisms such as direct tumor infiltration, neovascularity, cerebrovascular inflammation, and hemodynamic effects from high-flow vascular lesions (ie, arteriovenous malformations and fistulas) could trigger “neurovascular uncoupling” in those patients. Neurovascular uncoupling, and other pitfalls of fMRI, are briefly discussed.
David Mikulis discusses “neurovascular uncoupling syndrome,” where lack of functional hyperemia during neuronal activation can have long-term consequences on the integrity of the tissue in the absence of acute ischemia.
Jay Pillai discusses the successful clinical application of a technique to improve the consistency of BOLD fMRI by using a breath-holding technique.
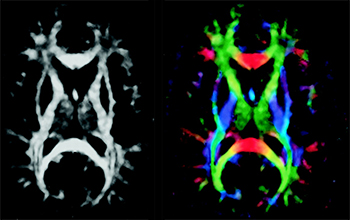
Aaron Field discusses the technique, clinical use, and some limitations of DTI and tractography, and describes patterns of alteration of white matter fiber tracts by neoplasms and other lesions.
Lastly, Wade Mueller shows that a neurosurgeon may obtain significant improvements in clinical outcomes and a drastic reduction in complication rates when working with a team that provides presurgical mapping of cerebral lesions by using fMRI and DTI (wisely, fully acknowledging their limitations) and when various team members clearly communicate using a common language.
Functional MRI and DTI are extremely useful techniques that have become increasingly available to neuroradiologists in recent years. As with any technique, these work best as parts of a whole. A good understanding of physiologic mechanisms is necessary to make us good “functional” specialists, and a good understanding of the limitations of any technique is necessary to make us better physicians.
Image modified from: Jellison BJ, Field AS, Medow J, et al. Diffusion tensor imaging of cerebral white matter: a pictorial review of physics, fiber tract anatomy, and tumor imaging patterns.
美德醫(yī)療深耕醫(yī)療設(shè)備研發(fā)制造多年,憑借對臨床需求的精準(zhǔn)洞察與前沿技術(shù)的持續(xù)攻關(guān),在醫(yī)療技術(shù)創(chuàng)新賽道穩(wěn)步前行,已成為兼具技術(shù)深度與行業(yè)口碑的醫(yī)療企業(yè)。6月,美德醫(yī)療火力全開,接連亮相香港理工大學(xué)UBSN神經(jīng)科學(xué)會議&研討會、廣東省醫(yī)學(xué)會第14次影像技術(shù)學(xué)學(xué)術(shù)會議、湖南省醫(yī)師協(xié)會放射醫(yī)師分會2025年學(xué)術(shù)年會…以硬核產(chǎn)品與創(chuàng)新方案,點燃展臺人氣,收獲行業(yè)高度關(guān)注!神經(jīng)科學(xué)前沿:香港理工大學(xué)UBSN會議在香港理工大學(xué)UBSN神經(jīng)科學(xué)會議&研討會上,美德醫(yī)療聚焦神經(jīng)科學(xué)領(lǐng)域需求,攜fMRI腦科學(xué)整體解決方案參展。模擬磁共振系統(tǒng)助力受試者提前適應(yīng)掃描環(huán)境,腦功能視聽覺刺激系統(tǒng)可精準(zhǔn)呈現(xiàn)刺激任務(wù)誘導(dǎo)特定腦區(qū)激活,磁共振腔內(nèi)監(jiān)測系統(tǒng)則實時保障數(shù)據(jù)質(zhì)量。三者協(xié)同發(fā)力,為任務(wù)態(tài) fMRI 研究與診療提供全流程支持,助力神經(jīng)科學(xué)邁向更精準(zhǔn)、高效方向。影像技術(shù)盛會:廣東省醫(yī)學(xué)會影像技術(shù)學(xué)會議廣東省醫(yī)學(xué)會第14次影像技術(shù)學(xué)學(xué)術(shù)會議現(xiàn)場,美德醫(yī)療以“專業(yè)影像配套設(shè)備提供商”身份亮相現(xiàn)場,其國內(nèi)率先通過NMPA認(rèn)證的磁共振病人監(jiān)護(hù)儀成為全場焦點。這款設(shè)備突破傳統(tǒng)監(jiān)護(hù)儀在強(qiáng)磁場環(huán)境下的應(yīng)用限制,通過特殊屏蔽技術(shù)與抗干擾設(shè)計,實現(xiàn)磁共振檢查過程中對患者生命體征的實時監(jiān)測,對危重患者、鎮(zhèn)靜中的小兒患者、麻醉病人等特殊情況下進(jìn)行的磁共振檢查而言,為醫(yī)療安全提供了堅實保障。圍繞新產(chǎn)品新技術(shù)新應(yīng)用,美德團(tuán)隊積極與臨床及一線學(xué)者展開深度交流,共同推動影像技術(shù)的進(jìn)步與發(fā)展。專業(yè)培訓(xùn)學(xué)術(shù)賦能:第十五屆《MRI 信號分析與圖像解讀》高級培訓(xùn)班與北京友誼醫(yī)院合作舉辦的MRI信號分析與圖像解讀培訓(xùn)班已延續(xù)至第十五屆,組織培養(yǎng)了近萬名放射科醫(yī)生參與深度學(xué)習(xí)及交流,一直由美德醫(yī)療全面負(fù)責(zé)項目的運行服務(wù)工作,為歷屆培訓(xùn)班的順利開展保駕護(hù)航。本次培訓(xùn)班匯聚了國內(nèi)知名磁共振專家,課程設(shè)置精心,理論與實踐并重,致力于讓大家學(xué)有所成,攜手共進(jìn),為提升我國醫(yī)學(xué)影像水平、造福廣大患者而不懈努力!放射醫(yī)師年會:湖南省醫(yī)師協(xié)會放射分會年會6月27-29日,亮相湖南省醫(yī)師協(xié)會放射醫(yī)師分會2025年學(xué)術(shù)年會,美德醫(yī)療基于對放射醫(yī)學(xué)領(lǐng)域的持續(xù)深耕,精心呈現(xiàn)“磁共振被試監(jiān)測與監(jiān)護(hù)系列”,通過不同視野、不同刷新率滿足各應(yīng)用場景的定制要求,多種生理信號采集方式監(jiān)測患者生命體征,以及定制化軟件進(jìn)行眼動追蹤和頭動調(diào)整,實時監(jiān)測人物狀態(tài),提升掃描數(shù)據(jù)質(zhì)量,為放射醫(yī)學(xué)發(fā)展注入“美德力量”,協(xié)同發(fā)展放射診療質(zhì)量提升路徑。四場行業(yè)學(xué)術(shù)會議的精彩亮相,是美德醫(yī)療技術(shù)實力與品牌魅力的生動展現(xiàn)。未來,美德醫(yī)療將持續(xù)深耕醫(yī)療領(lǐng)域,以創(chuàng)新驅(qū)動發(fā)展,以技術(shù)為鑰,以客需為錨,以匠心為帆,為行業(yè)發(fā)展、醫(yī)療服務(wù)升級輸出更多價值,期待與您再次相聚!
在醫(yī)療科技領(lǐng)域,國產(chǎn)化創(chuàng)新力量正強(qiáng)勢崛起,不斷突破技術(shù)壁壘,改寫行業(yè)格局。美德醫(yī)療自主研發(fā)的磁共振病人監(jiān)護(hù)儀作為國內(nèi)國產(chǎn)無磁監(jiān)護(hù)領(lǐng)域率先通過NMPA注冊的產(chǎn)品,自上市以來成績卓著,僅半年便在數(shù)十家醫(yī)療機(jī)構(gòu)成功裝機(jī),掀起了無磁監(jiān)護(hù)設(shè)備國產(chǎn)化應(yīng)用的熱潮。自 2004 年成立以來,美德醫(yī)療便錨定磁共振專業(yè)配套產(chǎn)品研發(fā)方向,深耕細(xì)作二十余載。憑借一支勇于創(chuàng)新、專業(yè)務(wù)實的高素質(zhì)團(tuán)隊,在腦功能磁共振成像(fMRI)專業(yè)設(shè)備及技術(shù)研發(fā)生產(chǎn)領(lǐng)域披荊斬棘,積累了深厚底蘊(yùn)。此次磁共振病人監(jiān)護(hù)儀的問世,是公司在高新技術(shù)國產(chǎn)化征程中邁出的堅實一大步,打破了長期以來國外產(chǎn)品在該領(lǐng)域的壟斷局面,填補(bǔ)了國產(chǎn)空白市場,彰顯出強(qiáng)大的技術(shù)實力與創(chuàng)新魄力。部分裝機(jī)照片該監(jiān)護(hù)儀采用先進(jìn)磁兼容技術(shù),在強(qiáng)磁場環(huán)境下運行穩(wěn)定,精準(zhǔn)監(jiān)測患者血氧飽和度、血壓、脈率、灌注等關(guān)鍵生命體征,為磁共振檢查中的患者安全筑牢防線。在性能穩(wěn)定性、監(jiān)測精準(zhǔn)度、操作便捷性等方面表現(xiàn)出色,契合臨床需求,短短半余年,裝機(jī)用戶已覆蓋數(shù)十家醫(yī)療機(jī)構(gòu),遍布北京、上海、山西、陜西、四川、山東、江蘇、浙江、廣東等省份,以卓越性能和品質(zhì)贏得市場認(rèn)可!部分裝機(jī)照片未來,美德醫(yī)療將持續(xù)加大研發(fā)投入,立足國產(chǎn)化創(chuàng)新,推動技術(shù)與產(chǎn)品迭代升級,為醫(yī)療影像事業(yè)發(fā)展注入更多本土智慧與力量。同時,不斷提升產(chǎn)品質(zhì)量與服務(wù)水平,為廣大用戶打造更優(yōu)質(zhì)、全面的醫(yī)學(xué)影像配套解決方案。
2025年4月13日,由深圳市美德醫(yī)療電子技術(shù)有限公司主辦的第15屆Task-fMRI基礎(chǔ)培訓(xùn)班在深圳總部圓滿收官。來自全國各地醫(yī)療機(jī)構(gòu)、高校的臨床醫(yī)生、科研萌新齊聚鵬城,通過三天的理論實踐深度交融,完成對fMRI技術(shù)的系統(tǒng)性學(xué)習(xí),助力學(xué)員掌握fMRI技術(shù)的核心技能。培訓(xùn)班延續(xù)"理實結(jié)合、學(xué)科交叉"的特色,特邀深圳大學(xué)成曉君教授、王超教授等領(lǐng)銜授課。課程設(shè)置兩大核心模塊:基礎(chǔ)理論精講涵蓋fMRI原理、實驗范式設(shè)計及統(tǒng)計學(xué)應(yīng)用;實踐操作帶教覆蓋E-Prime任務(wù)編程、SPM數(shù)據(jù)處理全流程。注重培養(yǎng)學(xué)員的自主操作能力,使學(xué)員們能夠切實掌握Task-fMRI的數(shù)據(jù)處理方法,實現(xiàn)從零基礎(chǔ)到獨立完成數(shù)據(jù)處理過程。為響應(yīng)學(xué)員在教學(xué)過程中反饋的需求:結(jié)合核磁掃描及配套腦科學(xué)研究設(shè)備的操作使用,系統(tǒng)梳理fMRI實驗從設(shè)備操作到數(shù)據(jù)采集的全流程。吳杞柱博士帶領(lǐng)一眾學(xué)員觀摩了美德醫(yī)療一系列腦科學(xué)研究設(shè)備,詳細(xì)介紹了美德模擬磁共振(Mock MR)、磁共振多參數(shù)被試監(jiān)測系統(tǒng)以及腦功能視聽覺刺激系統(tǒng)在fMRI實驗中的使用,加深學(xué)員對task fMRI數(shù)據(jù)采集過程的理解。為期三天緊湊而豐富的教學(xué)及實操課程,讓一眾學(xué)員們表示受益匪淺,他們認(rèn)為這次培訓(xùn)干貨滿滿,不僅提高了自己的專業(yè)技能,還為今后的研究工作提供了有力的支持。未來,我們將繼續(xù)深耕腦智科學(xué)基礎(chǔ)研究領(lǐng)域,持續(xù)服務(wù)于客戶需求,致力于打造醫(yī)學(xué)影像醫(yī)學(xué)研用一體化平臺,為中國腦科學(xué)事業(yè)發(fā)光發(fā)熱!
繪成錦繡展舊歲,揄揚風(fēng)雅待新年。近日,美德醫(yī)療2024年度總結(jié)大會完美收官。年會上半部分,由部門領(lǐng)導(dǎo)依次匯報各部門年度工作,全面復(fù)盤項目進(jìn)度,匯總生產(chǎn)基本情況,盤點體系運營工作,歸總成本把控效用,分析市場趨勢變動,進(jìn)而結(jié)合公司戰(zhàn)略規(guī)劃及市場宏觀環(huán)境進(jìn)行2025年的工作部署。年會下半部分,多才多藝的美德人帶來了一場場精彩絕倫的文藝表演,《吉他串燒》展現(xiàn)了員工朝氣蓬勃、積極向上的精神風(fēng)貌,幽默詼諧的脫口秀更是引得全場笑聲連連,掌聲雷動。最后,由總經(jīng)理湯潔女士壓軸點評與總結(jié),回望2024年的發(fā)展歷程,美德醫(yī)療始終本著客需為本、品質(zhì)為先的發(fā)展理念,致力于專研更精尖的產(chǎn)品,拓展更專業(yè)的技術(shù)領(lǐng)域,完善產(chǎn)學(xué)研用一體化平臺,打造更完整的醫(yī)學(xué)影像整體解決方案。未來,也將繼續(xù)用心服務(wù)每一位客戶,譜寫2025年“奮進(jìn)”新藍(lán)圖!
都說北京的秋天是出了名的美好,老舍先生也說:秋天一定要住北平。我們心心念念了一整年,大Boss一聲令下,我們出發(fā)啦! 11月18日,美德同事一行40人,帶著南國的熱情,從一個只有夏天和冬天的城市,以深圳的速度和激情,飛抵四季分明的北京,一同領(lǐng)略北國的秋韻。 北京的秋天果然很美,美得出乎意料,瓦藍(lán)的天空將整個城市映襯得干凈而清朗,金黃的銀杏葉燦爛奪目,驚起南方大小土豆“哇”聲一片,深秋的暖陽透過紅葉的縫隙照射到行人臉上,人們的笑容是如此陽光明媚……我們參加升旗儀式,感受國歌的莊嚴(yán)和力量;我們登天安門城樓,感受歷史的厚重與嚴(yán)肅;我們瞻仰人民英雄紀(jì)念碑,緬懷先烈的勇敢無畏;我們在天安門廣場踱步,回望歷史長河,感嘆中華文明。我們熱淚盈眶,我們躊躇滿志,我們自豪驕傲。何其有幸,生在春風(fēng)里,長在紅旗下。我們驕傲,因為我們是中國人!俯瞰神州大地,目光所至,皆為華夏;五星閃耀,皆為信仰。 當(dāng)五星紅旗隨著太陽徐徐升起的那一刻,愛國情懷已深深植根于我們每個人心間,它將生生不息,代代相傳。 走進(jìn)故宮,其巧妙的結(jié)構(gòu)、華麗的造型、博大的氣魄,無一不展示著古代皇權(quán)的霸氣和自信,讓人感到無比震撼。故宮的藝術(shù)之美,歷史之美,文化之美,舉世無雙。圓明園,這里的湖泊、假山和古建筑,共同演繹著和諧之美。坐上時光巴士,一幅幅流動的畫卷,讓人仿佛回到三百年前,自己就是那宮廷院內(nèi)的一員,沉浸式體驗了穿越歷史的樂趣。這里匯聚了自然之美、藝術(shù)之美和精神之美。漫步圓明園,感受歷史的厚重與歲月的沉淀,每一處都是故事,每一景都是回憶。秋天的長城,猶如一條蜿蜒的巨龍,盤旋在群山峻嶺之間,披著金色的霞光,沐浴在涼爽的秋風(fēng)中。長城之上,步步皆歷史,磚磚顯風(fēng)華,攀登之間,感受千年滄桑。太陽照,長城長,長城雄風(fēng)萬古揚。中國軍事博物館—軍事之翼,博物館里展翅,榮耀之光熠熠生輝。館內(nèi)各種模型、圖片和實物,將戰(zhàn)爭的殘酷和城市的堅韌展示得淋漓盡致。站在這些展品前,你會不禁為那些捍衛(wèi)和平的勇士們感到自豪,并深深體會到保家衛(wèi)國的重要性。雍和宮的每一座大殿、每一尊佛像、每一道門檻,都是歷史的沉淀和文化的傳承,這里的一景一物,無不在訴說著一個時代的輝煌。 歷史文化之旅, 國子監(jiān)是必去之地,它被譽(yù)為中國古代最高學(xué)府。在這里的每一步行走, 都似在與古人先賢對話,你能強(qiáng)烈感受到古代崇文重教的氛圍,以及古代學(xué)術(shù)的繁榮與嚴(yán)謹(jǐn)。游玩是生活的調(diào)味劑,但工作的責(zé)任心始終掛在心頭,這不是負(fù)擔(dān),是美德人的情懷和使命。 抵達(dá)當(dāng)晚,同事們顧不上早起的疲憊和一路奔波的辛苦,饒有興致地參觀了中科院生物物理所腦與認(rèn)知國家重點實驗室。美德公司成立至今,已有多款產(chǎn)品應(yīng)用于中科院腦科學(xué)研究試驗。同事們與相關(guān)專家進(jìn)行了深入的技術(shù)交流,這種面對面的溝通有利于我們改進(jìn)產(chǎn)品,提升品質(zhì)和更好地服務(wù)祖國醫(yī)學(xué)科研事業(yè)。我司與清華大學(xué)生物醫(yī)學(xué)影像中心也已合作多年,20日下午,同事們帶著激動的心情走進(jìn)這座神圣的高等學(xué)府,在研究中心實驗室和老師們進(jìn)行了熱切而實質(zhì)的交流。切磋完畢,同事們漫步清華校園,盡情地吸取這座智慧殿堂帶來的榮耀和力量。觀光旅游的同時兼有學(xué)術(shù)交流,此行簡直不要太超值。能為中國醫(yī)學(xué)事業(yè)做出自己應(yīng)有的貢獻(xiàn),美德人當(dāng)仁不讓。提高中國醫(yī)療科研水平,我們深感責(zé)任深重;展望未來,我們信心滿懷。 游頤和園,觀天壇,打卡恭王府,我們在景山公園探尋歷史足跡,我們在北海公園信步,漢服體驗,我們在后海的巷子里閑逛,品嘗北京小吃,我們在德云社里聽相聲……我們沉醉于長安街的華燈初上,又被鳥巢和水立方的璀璨燈光所驚艷,我們驚嘆于國家大劇院的夜景,又在前門大街的暮色里探尋……大鴨梨餐廳的北京烤鴨,油亮酥脆的外皮和柔嫩多汁的鴨肉相得益彰,色香味俱佳。咬一口,那酥皮流出的油脂在舌尖瞬間流轉(zhuǎn),香氣四溢,每一口都是對中華美食的敬仰。 東來順的涮羊肉,熱氣騰騰,暖胃更暖心,團(tuán)隊圍坐,笑語連連,推杯換盞,同事情誼在這一刻悄然升溫。 此次北京之行歷時5天,既是團(tuán)建,也是一趟愛國主義教育之旅,還是一趟飽覽中華五千年文明歷史的文化之旅;既是旅游,也是游學(xué);既是游玩,順帶工作,行程豐富,收獲滿滿。 揮別北京,那胡同里斑駁的墻,紫禁城里威嚴(yán)的梁,天安門前的紅旗飄揚,故宮深院的悠長,一幕幕在眼前回蕩,京城之行皆是華章。團(tuán)隊相伴凝聚力量,為夢續(xù)航。 盼與美德攜手共赴新程,再書佳績!
 關(guān)注公眾號
關(guān)注公眾號
 ? 2021 深圳市美德醫(yī)療電子技術(shù)有限公司 版權(quán)所有粵ICP備2022124818號互聯(lián)網(wǎng)藥品信息服務(wù)備案編號:粵網(wǎng)藥信備字(2025)第00866號
? 2021 深圳市美德醫(yī)療電子技術(shù)有限公司 版權(quán)所有粵ICP備2022124818號互聯(lián)網(wǎng)藥品信息服務(wù)備案編號:粵網(wǎng)藥信備字(2025)第00866號